Is Vanga demographically trapped?
By M. H. King, University of Leeds
Figure 1 - Congo Kinshasa. Vanga lies on the lower edge of the central rainforest area.
Background
In
1912
the American Baptist Mission Board set up a station at Vanga on the Kwilu river
in what was then the south/central region of the Belgian Congo, and what is now
the Democratic Republic of Congo (also known as D. R. Congo or Congo
Kinshasa).
The medical work was local, and entirely curative until 1962 when vigorous expansion began. Whereas previously, the one mission doctor saw all patients himself, there was now intensive staff training, first of nurses, male and female, and later of workers of many kinds, so that tasks could be delegated to them. Health centers and village clinics were set up, and a vigorous attempt made to decentralize authority, so that the community feel that they not only manage their various health units, but also that they own them. This was accompanied by a program of preventive care, including particularly the provision of safe water and sanitation.
Progress was such that by 1980 it was decided that the pattern of care developed at Vanga should be used as the pattern for the entire Congo, which was divided into 50 Health Zones in a national program of Rural Health or SANRU. This system is commonly reckoned to be among the best in Africa, if not the best.

Figure 2 - Vanga hospital. The Kwilu river is in the foreground, with Vanga Cité in the background.
Meanwhile by 2002 Vanga hospital itself with its daughter hospital at Sala had grown to 400 beds with a total of 563 health staff in the zone as a whole, including 17 doctors (one expatriate).
From 1962 until 1997
the hospital at Vanga was run by a very distinguished missionary Dr. Dan
Fountain - 'Fontaine' to the locals, and immensely respected. In May
2003 I had the privilege of staying with Dan, recently retired to Tennessee. As
we prayed over breakfast, I said I always prayed for "the trapped"
and for almost nobody else! After a few moments silence, Dan said: "Come
to Vanga!"
The upshot of this was that in August I presented an account of demographic entrapment to a meeting in Kinshasa - Pièges demographiques au Congo? This was organized by SANRU for the leaders of the Congo's health zones. There was no sign of a taboo, or indeed of any anger, and much interest, particularly in Les Démons!
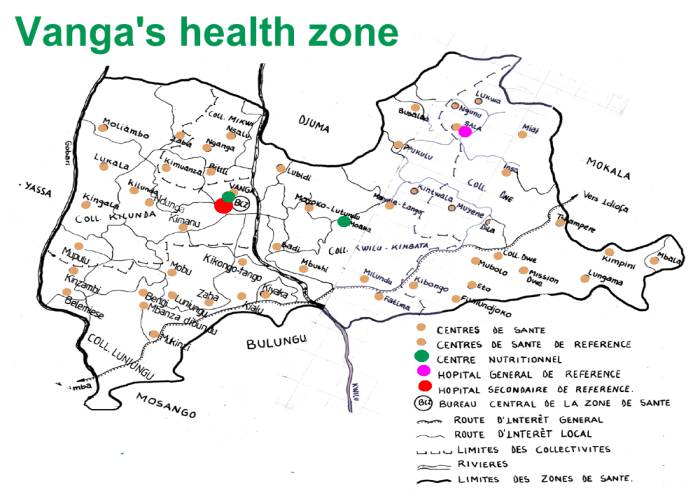
Figure 3 - Brother George's map of Vanga's health zone. Note that it stretches across the Kwilu river.
Mercifully, whatever might be the case in the North, the taboo on demographic entrapment does not appear to exist in the D. R. Congo! At this meeting the representatives of the Congolese government were urged to "bang on the tables" of UN meetings and to ask: “What is it demographic entrapment? Help us!” in the hope of lifting the taboo in the UN agencies, so as to provide assistance for disentrapment, not only in the Congo, but also elsewhere in Africa, as suggested by Figure 'X'.
If the South has to reduce its fertility to avoid starvation and violence, the North will be expected to reduce its resource consumption and live sustainable lifestyles (Demon 3) - to the enormous benefit of the world as a whole in view of the danger of global warming. It is therefore of the greatest importance, both to the North and the South, that the taboo be lifted and that many people bang very hard on the conference tables, as well as making a formal requests to the UN agencies: “What is it demographic entrapment? Help us!”
When
the SANRU meeting was organized it was generally assumed that the Congo is not
demographically trapped, but that it was high time that people started thinking
about it.
However, further examination of the situation suggests that much of it may have reached the 'warning stage' in the definition below, and that Vanga has reached 'the definitive stage'. If so, the most urgent steps need to be taken to reduce human fertility with all possible speed.
Besides Vanga, the other areas that appear to be at particular risk include the North Kivu, which the Belgians had long considered trapped {122} and ??? [Dan, do fill in the areas you are worried about as seen from the air].
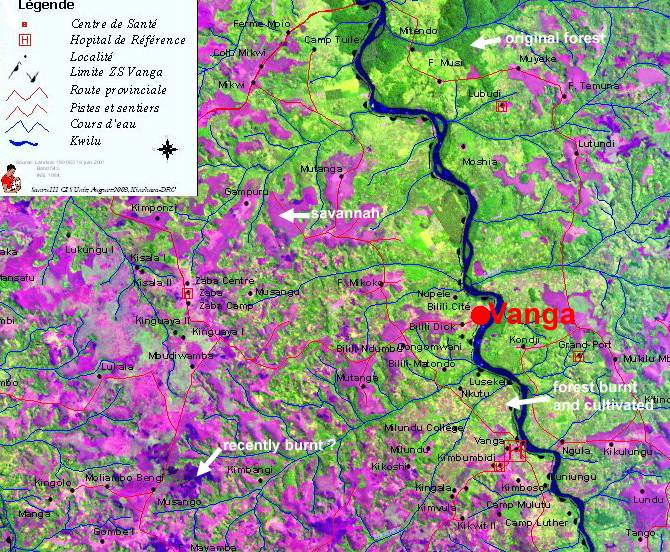
Figure 4 - A satellite map of Vanga. (1) Purple - savannah. (2) Dark blue - recently burned savannah. (3) Dark green -untouched rain forest. (4) Mottled yellow green converted to cultivation, now showing crops in various stages, with areas in various stages of fallow. Note that very little of the original forest remains.
Definition of entrapment
Demographic entrapment is considered to have a definitive stage and an earlier warning stage:
Definitive stage. A community is demographically trapped if it exceeds: (a) the carrying capacity of its ecosystem, and (b) the ability of people to migrate, and (c) the ability of its economy to produce sufficient goods and services which it can exchange for food and other essentials.
The end-result of entrapment is the direst poverty, starvation (famine), and violence.
Warning stage. A community is also demographically trapped, if, because its population is increasing, it is expected to reach the definitive stage with starvation and violence before long.
Demographic entrapment is taboo, in that it is never discussed by demographers, by development economists, or by the UN agencies. The reasons for this taboo (the so-called Hardinian taboo) have been called its 'Demons'. {168}
What then is the evidence of that Vanga is demographically trapped? And if so,
in what stage is it in, and what might be done about it?
Vanga lies at the southern limit of the central rainforest area of the Congo, where it borders on the savanna. Its many little river valleys where once densely forested, with sharp borders between the forest and the largely treeless savannah between them.
Vanga’s health zone straddles the Kwilu river. To the west of the river it is largely Mbala, Songo, Hungana, and Humbu. To the east it is almost entirely Yansi.
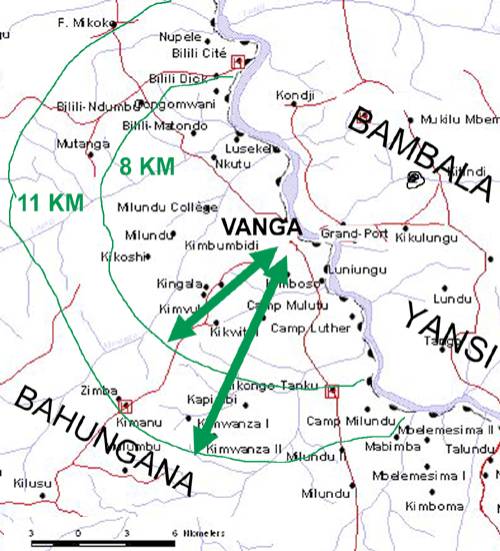
Figure 5 - How far do villagers now have to walk? The villagers of Vanga now have to walk between 5 and 11 km to their gardens. Since they are mostly Bahungana, they cannot cross the river into the territory of the Yansi.
Ethnography
Early in the first millennium the pygmies of the Congo forests where progressively replaced by Bantu peoples from West Africa with the result that there are now about 500 tribes with as many largely distinct languages. These tribes are generally very reluctant to share their land with anyone else. Before the arrival of the Belgians in 1880 there had been cannibalism in the Vanga area. Since then, the traditional culture of the area, including its arts and crafts, has progressively disappeared.
Population
The rising fertility with the coming of modernization that has been documented for other parts of Africa appears to have been true for the Congo, and to have contributed greatly to population increase. For example, the tradition of a newly delivered mother returning to her village with her baby and staying there until he can walk has largely gone. This would have had a powerful effect in spacing births and slowing population increase.
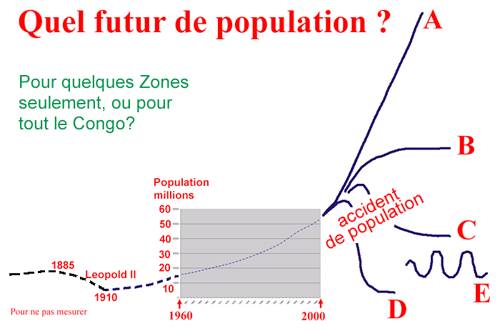
Figure 6 - Future population patterns for the Congo? While the Congo was owned by King Leopold
population seems to have fallen. It increased from 12 million in 1960 to 50
million in 2000. There are various future possibilities. A. Exponential increase. This seems unlikely in view of what is said
below about carrying capacity. B. Further rise followed by a steady state. C. A population crash followed by a steady state. D. A steeper population crash followed by a steady state. E. Oscillations. Many other curves are possible, so are combinations
of them.
Population growth in the Vanga Health Zone has followed that in the Congo as a whole, as shown in Figure 6. This has now reached the point that by 2002 there were 70 people per sq. km or 0.7 people per hectare 1 - much denser than for the Congo as a whole for which the corresponding figures are 21 people per sq. or 0.21 people per hectare. In the immediate vicinity of the hospital population densities have reached 110 people per sq. km. How far the health units of Vanga are responsible for the increase population density compared with the rest of the Congo, is not known.
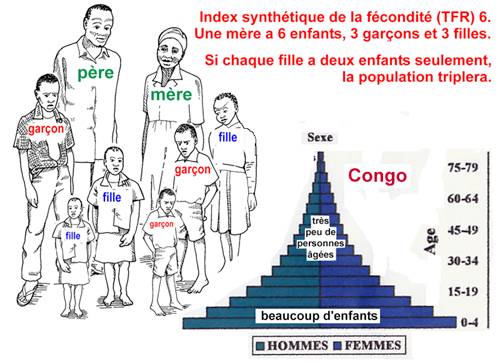
The total fertility rate for the Congo as a whole is 6.4 2 (6.4 children per mother) with 40 % of the population under 15. The rate of natural increase of the population is 3.4%, which implies that the population will double in 20 years.
|
|
|
|
|
|
{kind=link}
Figure 7 - Population
(demographic) momentum - l'elan demographique. This is
daunting indeed and is why there are demographers who will say - privately -
that the population scene in Africa is terrifying!
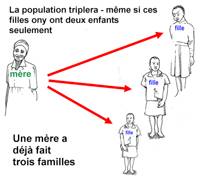
A total fertility of 6 implies that the average family has six children, or on average three sons and three daughters. Whereas there is one family now, the fact that there are already three daughters implies that the population would triple - even if every female where to have two children from now on. The fact that the population can be expected to at least triple - indeed it can be expected to much more than triple - implies that, although a community might not have surpassed the present carrying capacity of its ecosystem, and reached the definitive stage of entrapment, it could well have reached the warning stage, so that it exceeds the carrying capacity of its ecosystem in the near future.
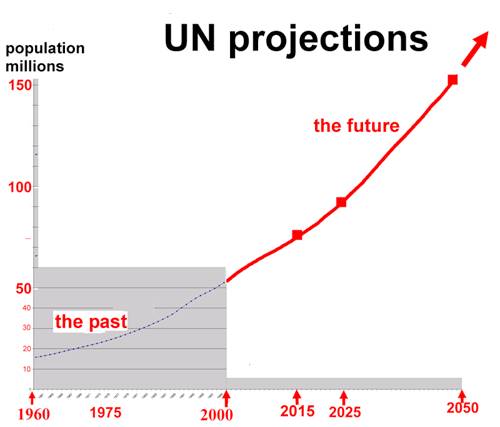
Figure 8 - Population forecasts for the Congo. The Congo's present population is 52 million. It is projected to increase to 74 million in 2015, to 95 million in 2025 and to 151 million in 2050.
Family planning. Most recent annual reports for the health zone make no mention of family planning. However, the report for 1998 records 5000 family planning attendances, with 4.7% of couples using a modern method, mostly pills, injections, and condoms with occasional tubal ligations, and no vasectomies.
AIDS. Since the prevalence of HIV among adults is only 5% in the Congo, it is unlikely to have any noticeable effect on population increases - unlike the situation in many other parts of Africa.
Economic development. After a long period of economic retrogression, particularly during Mobutu's regime, [What were his dates?] and several wars, the Congo now seems set for a it most fruitful period off peace and economic development.
Vanga has seen the closure of its palm oil extraction plant, the decline of
river transport, and such for grave deterioration of the roads as to virtually
if cut it of from Kinshasa and the rest of the country.
Agriculture
In the 16th century [?] the Portuguese introduced manioc (cassava) from South America, which has progressively replaced the yams and millets that are traditional to the area.
Manioc is such an efficient source of food energy, particularly in poor soils, that it has greatly increased the Congo's carrying capacity for man, and has made it possible to support a much denser population, with the minimum of labor. The present population explosion in Africa is largely the gift of manioc and maize, which was also introduced from South America.
Agriculture is entirely by hand hoes. There are no draught animals ploughs, or carts. Most goods are carried on the heads of villagers, usually women. Agriculture in Vanga is still in the Iron Age.
In principle, there are two sustainable methods of agriculture, cut and burn or agroforestry.
Cut and burn. In a tropical forest most of the nutrients part in
the biomass, so the common way to make
use of them is to cut down the trees of the forest, burn them, and plant
crops in the ashes for two seasons, after which
the plot is abandoned and allowed to remain fallow
for 18 years. By this time the forest will have returned, and can be burnt
again. Unfortunately the long fallow periods imply a low carrying capacity in terms
of persons per hectare. Lack of land is
increasingly making it impossible to allow the long fallow periods that are
required to maintain soil fertility. The result is that fallow periods are
becoming increasingly short, and soil fertility is progressively falling.

Figure 9 - A 20-year fallow. Unfortunately, fallow periods are often much shorter than this and are often continuous.
Agroforestry. This is carefully chosen patterns of mixed crops, usually a nitrogen fixing leguminous shrub and a food crop. The difficulty with agroforestry is that it is commonly considered too difficult for the simple villager, and requires too much foresight. It also needs careful testing and a dedicated cadre of extension workers to introduce it widely. Agroforestry is being researched at the agricultural research station at Lusekele in the Vanga health zone, but is not yet sufficiently advanced for widespread introduction. (Ed Noyes, do please correct and fill this section).
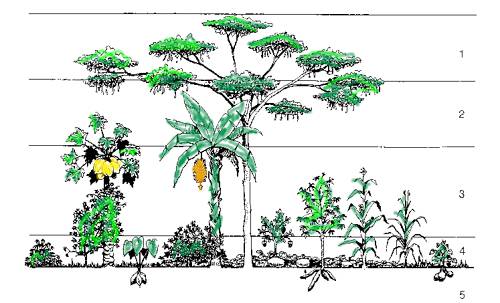
Figure 10 - Agroforestry. The important principles are mixed crops, particularly with the trees and legumes. They need to be carefully adapted to particular situations, and are not easy to manage.
Carrying capacity is highly dependent on the fertility of the soil. Most soils in the Congo are of low fertility, with a low cation exchange capacity (ability to retain potassium and phosphate, etc.), and have been thoroughly leached, in that most essential nutrients have long been washed away. They also have high soil temperatures, which promote the oxidation of organic matter with the result that little is left in the soil to encourage the entry of roots, and the retention or water etc. They thus provide a formidable agricultural challenge when it comes to providing the maximum number of calories for food energy for the increasing number of people that each hectare has to support.
There are two types of land the high forest bordering the rivers, and the savannah grasslands between the river systems. The villagers burn both. They burn the almost completely infertile savannah to catch rats and small game. They burn the forest to plant in the ashes.
Since maize and dry cassava have almost identical energy values the figure of 250 kg per year can be used for both of them.
For maize the best women get 700 kg/ha and average ones only 600 kg/ha (Ed Noyes at Lusekele, near Vanga). Assuming an average value of 600 kg, 250 kg is produced by 0.4 ha. A family of six children and two parents therefore need 8 x 0.4 = 3.2 ha without allowing for a fallow period. Allowing for a year's fallow, this is about 6.4 ha per family per family of 8, or or 0.8 ha per person.
For cassava an average figure for Africa is 5-7 tons of fresh cassava to the hectare, say 6 tons (Barry Pound, personal communication). This is equal to 2.1 tons of dry cassava. Assuming a yield of 2.1 t/ha, 250 kg are produced on 0.12 ha. A family of six children and two parents therefore need 8 x 0.12 = 0.96 ha without allowing for a fallow period. Allowing for a year's fallow, this is about 2 ha per family of 8 or 0.25 ha per person.
Since there are 0.7 ha per person in Vanga's Zone du Sante, land area per head should be no problem, if it were all cultivable. However, no figure is available for the proportion which is forest, and that which is savannah. Looking at the satellite map in Figure 4, let us assume that half of it is cultivable forest and that the rest is uncultivable savannah. If so there are 0.35 cultivable hectares per person.
This is getting
uncomfortably close to the 0.25 ha which are theoretically necessary. It only
requires moderate inequality in land-holdings, or moderate export of cassava,
for there to be real land shortage and malnutrition.
Starvation (malnutrition). Rising malnutrition rates are an indication of entrapment. There has always been some of malnutrition at Vanga, at least since 1962. However, several recent annual reports list malnutrition as the major problem, and that for 1998 includes a graph showing its steady increase over the previous ten years. [Brother Freidheim - what proportion of the malnourished children are older - say 6 or 7 - because this in an indication of severe food shortage?]
Violence. There are reported to be an increasing number of
wounds needing surgery that result from disputes over land. This is a serious
sign of land scarcity.
Migration. It is said that none of the 500 tribes of the Congo
are willing to share their land with any other. The possibilities for migration
would therefore seem limited.
In particular the
Bahungana east of the Kwilu river are unwelcome among the Bambala and Yansi
west of the river.
Conclusion
Assuming that Vanga can just about support its present population (highly optimistic considering current land shortage and ecological destruction) and yet it's population could be expected to triple, even if all mothers had two children only from a now on, they should ideally have one-child families with the greatest urgency.
Since
mothers are at present unwilling to consider any reduction in the number
of their children, this is obviously quite impracticable. Nevertheless, it is a
dialogue that ought to begin among les intellectuels de Vanga, in the
hope that in future years it will become more practical, and will, in some
measure, diminish the starvation and violence that can be expected.
Theology
Since Vanga is a Christian mission hospital, and the whole community fervently Baptist, and with Dieu on everybody's lips, and in everyone's souls, it is surely necessary to pray about what God really wants for Vanga.
Having long prayed for the trapped in general, and now for Vanga in particular, it is most important pray about the extent to which a human action is necessary to complement the Divine will. From the perspective of a "prayer book Anglican" I pray that everything humanly possible be done to prevent the starvation and violence that seem likely to befall Vanga. To do nothing is surely fatalism.
All disasters - even this one - have a positive aspect. The positive side here is for the disentrapment of Vanga to be a model for the rest of Africa. There is no knowing what is in the Divine will. One possibility is an influenza pandemic with a high mortality, North and South. Another is catastrophic global warming.
Nevertheless, there are disasters we can do something about, and the starvation and violence of entrapment is surely one of them.
So what next?
The first step is surely for the
Government to ask the various UN agencies: "What is this entrapment we
hear it but? Can you assist us?" This would rapidly lift the taboo on
entrapment in the UN agencies, and would be of the greatest help to the Congo,
to Africa, and to the world in general.
The next step is to make high-quality
family planning services available to all the villagers. This requires the
provision of adequate family planning supplies and the further training of
health staff.
The third step is for the problem to be
discussed by its the community. The pastors seem likely to be the key link to
the community, so urgent steps should be to discuss it with them. Somehow a
discussion has to be started on these lines: "If we go on having many
children, they and we are going to starve. Somehow we must have few children.
What can we do about this?"
I will try to produce the draft of some teaching materials in French, and get these out to you soonest.
Editorial notes
FIRST DRAFT: the idea is that this website be the basis of several papers, hopefully with many authors, with my own at name last, if it appears at all.
Where I am unsure of names or data, I have guessed, in the assurance that my many errors will be corrected.
If you want an e-mail version on which to make corrections, do let me know. Make corrections in the text, return it by e-mail, and I will send you a corrected version. Be brutal! Say what you really think! Don't worry about grammar or style - I will fix that! I will also tidy-up the illustrations. My email is M.H.King@leeds.ac.uk.
At present it is not designed for any specific journal, the intention being that a long paper, with many detailed endnotes, be available on the web, in French and English, and that extracts be put into various journals, probably Tropical Doctor, and with luck The Lancet. Since entrapment is presently taboo to The Lancet, this will take some doing! It will need to be carefully styled for each journal.
Unless anybody else wants it, I intend to leave it on the disentrapment website here at the University of Leeds. I have put various French words (piège demographique, depiègization), etc. into the metatext, so that Google will find them. I also hope to have some other French translations on the website. I very much hope that we will have a continuing dialogue on the website with 'les intelectuels de Vanga' and others. If any other website would like it, do have it.
Since the Vanga experience of depiègization is only just beginning, it is in effect, a baseline paper and will hopefully be the first of a series which will report future progress.
If it would be useful for me to revisit Vanga, I would be happy
to do so at almost any time, and at my own expense.
Data needed
The population densities of all the health zones, etc.